When sending out monitoring invites, there are two folders to choose from:
2e Invites I Monitoring I All
2f Invites I Monitoring I Priority Only
You may wonder why we have different sections at all, why not just group them all together?!
All practices experience variability in their capacity and have times when they need to focus on higher-priority invites first. The two folders include different sets of reports to help you prioritise.
- All
HRD (High Risk Drug Monitoring)
This set of reports includes shared care Drugs, other high risk drugs that require frequent monitoring, overdue critical annual monitoring, and critical tests after starting new medication.
RM (Routine Monitoring)
This set of reports includes frequent monitoring (more frequent than annual) and one-off requests. Essentially any patients who need either one-off or frequent monitoring and who aren't in the HRD reports above. This includes things like 6 monthly HbA1cs for diabetics, any regular monitoring that's been configured on individual patients, and any one-off requests set up using our templates.
- Priority Only
HRD-SC (High Risk Drug Monitoring - Shared Care Only)
This is the highest priority of the HRD section above.
MON-HP (High Priority Routine Monitoring Only)
This is the highest priority of of the RM section above, and includes PSA, one-off requests set up using our templates, and tests for diabetes diagnosis.
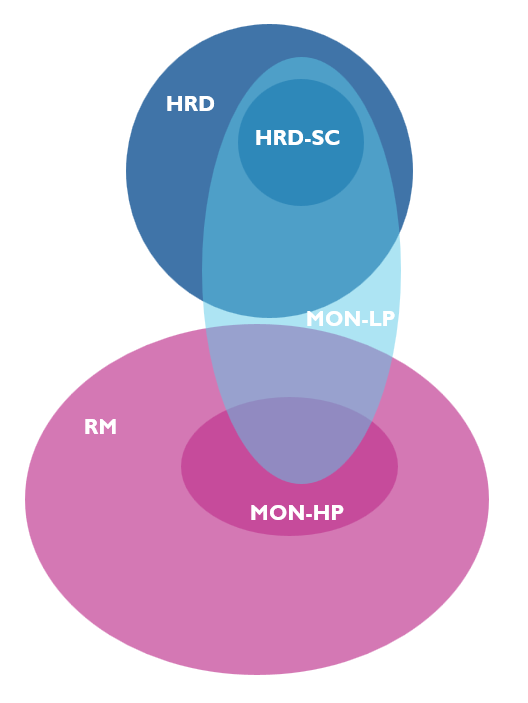
MON-LP (Localised Priority Monitoring Only)
This set of reports includes one-off requests set up using our templates, shared care drugs, medication changes requested to monitor and any Localised Priorities [see options below]
This diagram shows how the different monitoring sections overlap and relate to each other.
- If a practice has sufficient capacity, the reports below cover all the patients who need monitoring. Ideally, both of these sections should be sent each week.
HRD and RM in the folder 2e Invites I Monitoring I All
- If capacity is limited, the reports below can be used.
HRD-SC and MON-HP in the folder 2f Invites I Monitoring I Priority Only
- Alternatively if you want to choose your own priorities, the reports below can be used. They will always includes ad hoc requests, requests to monitor new medication and shared care drugs that require frequent monitoring. Other items to be included can be configured for each practice.
MON-LP in the folder 2f Invites I Monitoring I Priority Only
Here's more detailed information about what we mean by the terms in the list above:
Shared Care Drugs:
Any of these medications on repeat and not coded as monitored by Secondary Care:
- ADHD/CNS Stimulants (<18y)
- Antiproliferative immunosuppressants
- Azathioprine
- Ciclosporin
- Cinacalcet
- Dapsone
- Intuniv (guanfacine)
- Leflunomide
- Mercaptopurine
- Methotrexate
- Midodrine
- Rifaximin
- Sirolimus
- Sulfasalazine
- Tacrolimus
Other High Risk Drugs
Any of these medications that are on repeat and that require monitoring more frequently than annual:
- Alfacalcidol
- Amiodarone
- Antimetabolites
- Apomorphine
- Azithromycin
- Carbimazole
- Denosumab
- DOACs
- Dronedarone
- Gold salts
- Lithium
- Loop diuretics
- Minocycline
- Mirabegron
- Modafinil
- Nitrofurantion / Trimethoprim on more than 6m
- Oral Retinoids
- Penicillamine
- Potassium-sparing diuretics and aldosterone antagonists (Eplerenone / Spironolactone)
- Sulfasalazine
- Ursodeoxycholic acid
Overdue Critical Monitoring
These are medications that are very important to monitor annually and become high risk when that monitoring is overdue. These medications on repeat, without appropriate monitoring in the last 14 months are included in section 1:
- ACE/ARB
- Antipsychotics
- Digoxin
- DOACS
- Loop Diuretics
- Olsalazine, Balsalazide, Mesalazine
- Sodium Valporate
- Thyroid hormones
Critical tests after starting new medication
Historically, our systems identified these by looking at repeat medication. Now this is based on the pop-ups you see when starting or changing medication. Time frames depend on the medication and options selected on the pop-ups.
- Allopurinol / Febuxostat with no UE & Urate after starting / changing
- Anti-Hypertensives with no UE after starting / changing
- Statins or other Lipid Regulating agents with no ALT / LFT after starting
- Testosterone Replacement with no Testerone levels after starting
- Thyroid Hormones with no TFT after starting / changing
Local Priorities
These are practice dependent. These are the current options available:
- Bloods to repeat following abnormal results from pathology system
- Carbimazole Monitoring
- Diabetes Diagnosis (i.e. repeating one-off raised HbA1c)
- Diabetes Monitoring
- DOAC Monitoring
- PSA Monitoring (patient specific)
Just let us know if you'd like any of these enabling for your practice, or if there's another priority you'd like to request.
Was this article helpful?
That’s Great!
Thank you for your feedback
Sorry! We couldn't be helpful
Thank you for your feedback
Feedback sent
We appreciate your effort and will try to fix the article